HEPATIQ may be used by clinicians such as hepatologists, gastroenterologists and internists to assess the health of the liver for patients who test abnormal on blood tests or elastography. It is also of value to those managing liver cancer such as oncologists, interventionists and liver surgeons to assess liver functional reserve before an intervention or surgery. Scroll down for details about each specialty.
Hepatologists, gastroenterologists and internists
Hepatologists, gastroenterologists and internists manage patients with liver disease. They use blood tests, elastography and biopsies for diagnosis and prognosis. These are all fibrosis based assessments of the liver. However, the liver regenerates and blood flow to the liver increases to compensate for fibrosis.
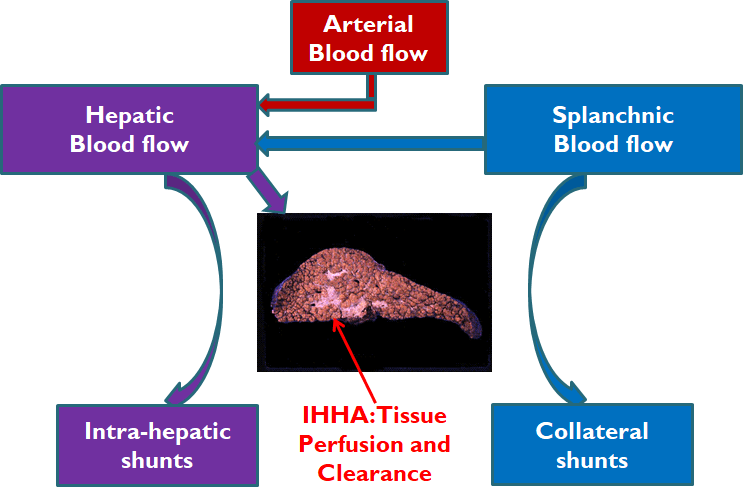
The liver gets its blood (hepatic flow) from the heart (arterial flow) and from the gut (splanchnic flow). Some of the splanchnic flow does not reach the liver due to collateral shunts. Some of the hepatic flow is effectively lost due to intra-hepatic shunts. These intra-hepatic hemodynamic abnormalities (IHHA) play an important role in tissue perfusion and clearance. [26] Fibrosis measurements entirely miss the IHHA of chronic liver disease.
Thus, an F4 or F3 patient may be H0 or H1 and may remain stable for years or decades. On the other hand, another F4 or F3 patient may be H2 or H3 and may be at risk of decompensation.
Furthermore, abnormal liver patients (>F0) may be sicker than the fibrosis measurement suggests [B,C]. For better diagnosis and prognosis, HEPATIQ may be used to assess liver functional reserve for abnormal liver patients (>F0) .
Oncologists, interventionists and liver surgeons.
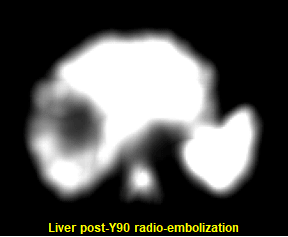
Liver transplantation (LT) has the greatest cure potential for hepatocellular carcinoma (HCC) patients. Bridge therapies prior to LT include stereotactic body radiation therapy (SBRT), Yttrium-90 radioembolization (Y90), radiofrequency ablation (RFA), transarterial chemoembolization (TACE) and surgical resection. The figure shows a SPECT image of the liver after Y90 therapy. Notice the dark region in the middle of the liver indicating the large volume of liver tissue (tumor and non-tumor) destroyed by the radiation.
A 2022 publication in The Journal of Hepatology, “The importance of liver functional reserve (LFR) in the non-surgical treatment of hepatocellular carcinoma” by D’Avola et al [D], discusses the role of LFR and efforts to estimate it. The paper concludes that “patients with compensated cirrhosis and large liver functional reserve can always receive the most radical treatment”. However, “a more detailed and individualized assessment should be carried out in patients with poorer liver functional reserve”. HEPATIQ may be used to assess the patient's liver functional reserve before an intervention or surgery.
LIVER FUNCTION
All of the blood leaving the stomach and intestines pass through the liver. The liver processes this blood and creates nutrients for the body to use. The liver also excretes bile which helps to break down fats, preparing them for further digestion. Life is not possible without a functioning liver. Infections, alcohol and fat build-up can affect liver function by causing the accumulation of fibrosis or scar tissue in the liver. Biopsies, elastography and blood tests measure or score liver fibrosis but do not quantify remaining function.
Patient outcomes are determined by the liver functional reserve, not the extent of fibrosis. This was established in the 8 year, prospective, multi-center HALT-C trial, which indicated that quantitative liver function is more accurate than staging fibrosis in predicting clinical outcomes. [5,6] Subsequent clinical research has further confirmed that function outperforms fibrosis in predicting outcomes. [12,13,16,17,21,22,24]
Liver functional reserve is measured by the perfused hepatic mass (PHM) with normal function being PHM>100. [4] A large, badly scarred, stiff liver can have normal function if there are enough functional nodules and adequate blood flow. Once a patient’s PHM drops below 75, they may decompensate, that is, develop clinical problems.[5,6,11,14,19,20,24] If their PHM falls below 60, they may die if not transplanted soon. [10,15,18]
The HEPATIQ report shows six indices: PHM (liver function), fLV (liver volume), fSV (spleen volume), HAI (alcoholic hepatitis), eFS (estimated fibrosis) and eEV (estimated varices). These indices are used for diagnosis, staging, interventions, and monitoring liver disease progression. They help identify those at risk of ascites, variceal bleeding, hepatic encephalopathy and liver-related death. [5,6,10,11,14,15,16,18,19,20,23,24,25,26] Differentials of these indicate steatotic liver disease, steatohepatitis, alcoholic hepatitis, cirrhosis, portal hypertension, varices and infiltrative spleen disease. [5,6,8,11,14,16,21,22,23,25] HEPATIQ also provides the H0-H5 physiological stage of liver disease. [27,28]
Comparative Analysis
.png)
Predictive ability of blood test based fibrosis scoring systems, such as APRI, FIB-4, NFS, etc., to identify persons with advanced fibrosis associated with development of cirrhosis is modest [B]. Fibrosis scores have poor sensitivity for predicting advanced liver disease in diabetic patients [C]. Elastography or a biopsy may be performed for staging liver disease (F0-F4) but they don't provide information on liver functional reserve. It may be beneficial to use HEPATIQ to assess liver functional reserve for patients designated as abnormal (>F0) [12,13,17,22]. Furthermore, before a liver surgery or any liver interventional procedure, use HEPATIQ to assess liver functional reserve [D].