HEPATIQ is useful to hepatologists, gastroenterologists, oncologists, interventionists, liver surgeons, nuclear medicine physicians and radiologists. Scroll down for details about each specialty.
Hepatologists, gastroenterologists and internists
Hepatologists, gastroenterologists and internists manage patients with liver disease. They use blood tests, elastography and biopsies for diagnosis and prognosis. These are all fibrosis based assessments of the liver. However, the liver regenerates and blood flow to the liver increases to compensate for fibrosis.
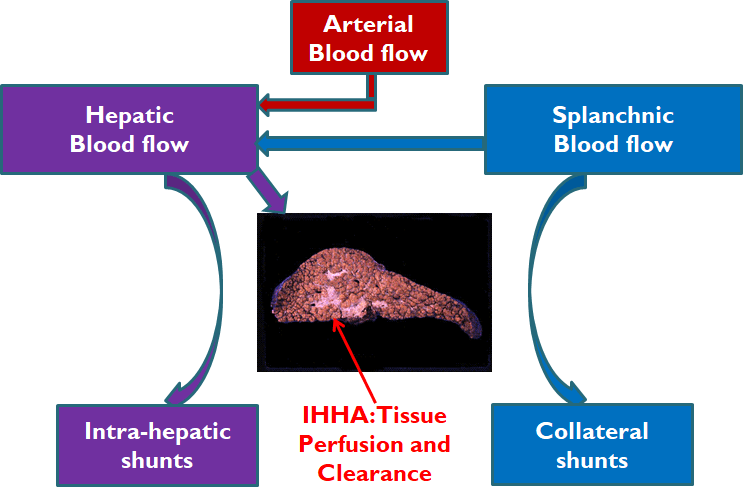
The liver gets its blood (hepatic flow) from the heart (arterial flow) and from the gut (splanchnic flow). Some of the splanchnic flow does not reach the liver due to collateral shunts. Some of the hepatic flow is effectively lost due to intra-hepatic shunts. These intra-hepatic hemodynamic abnormalities (IHHA) play an important role in tissue perfusion and clearance. Fibrosis measurements entirely miss the IHHA of chronic liver disease.
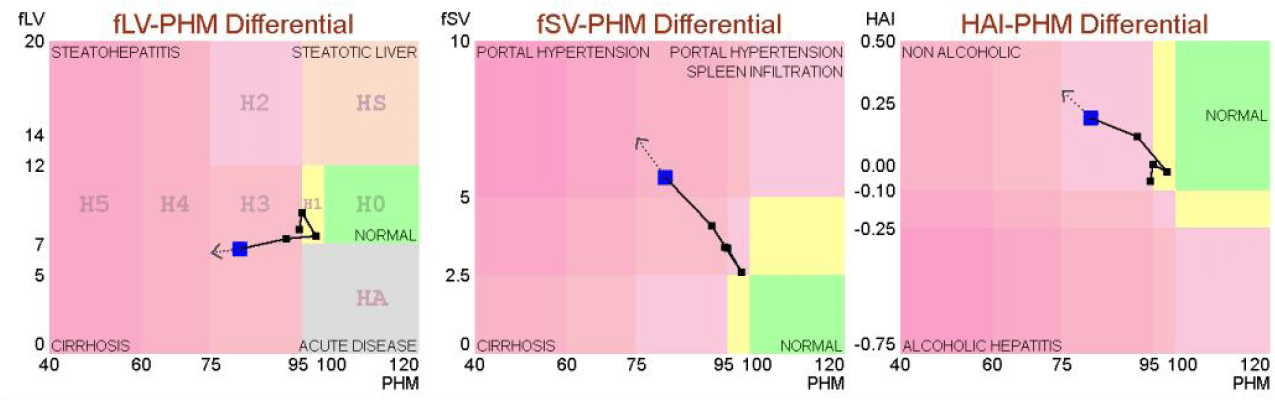
Thus, an F4 patient may be H0 or H1 and may remain stable for years or decades. On the other hand, an F4 patient may be H2 or H3 and may be at risk of decompensation.
Furthermore, abnormal liver patients (>F0) may be sicker than the fibrosis measurement suggests[A-B]. For better diagnosis and prognosis, HEPATIQ may be used to assess liver functional reserve for abnormal liver patients (>F0) .
Oncologists, interventionists and liver surgeons.
Liver transplantation (LT) has the greatest cure potential for hepatocellular carcinoma (HCC) patients.
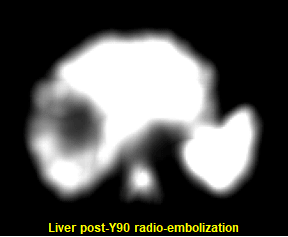
Bridge therapies prior to LT include stereotactic body radiation therapy (SBRT), Yttrium-90 radioembolization (Y90), radiofrequency ablation (RFA), transarterial chemoembolization (TACE) and surgical resection.
The figure shows a SPECT image of the liver after Y90 therapy. Notice the dark region in the middle of the liver indicating the large volume of liver tissue (tumor and non-tumor) destroyed by the radiation.
A 2022 publication in The Journal of Hepatology, “The importance of liver functional reserve (LFR) in the non-surgical treatment of hepatocellular carcinoma” by D’Avola et al [C], discusses the role of LFR and efforts to estimate it. The paper concludes that “patients with compensated cirrhosis and large liver functional reserve can always receive the most radical treatment”.
However, “a more detailed and individualized assessment should be carried out in patients with poorer liver functional reserve”. HEPATIQ may be used to assess the patient's liver functional reserve before an intervention or surgery.
patient Case studies
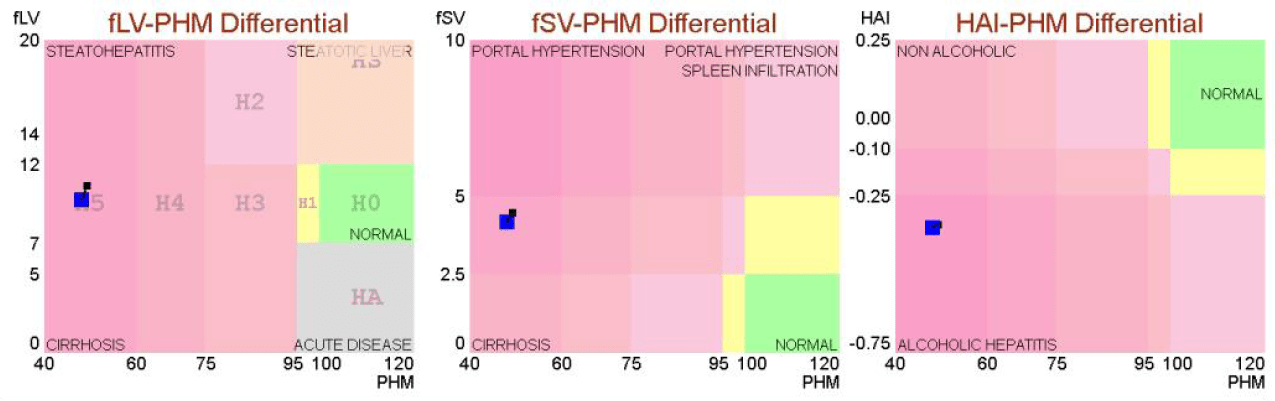
CASE 1 - H5 alcoholic hepatitis patient died. 53 year old female presented with PHM 48 (H5). HAI -0.35 indicated marked alcoholic hepatitis activity. Patient died soon after hospital admission.
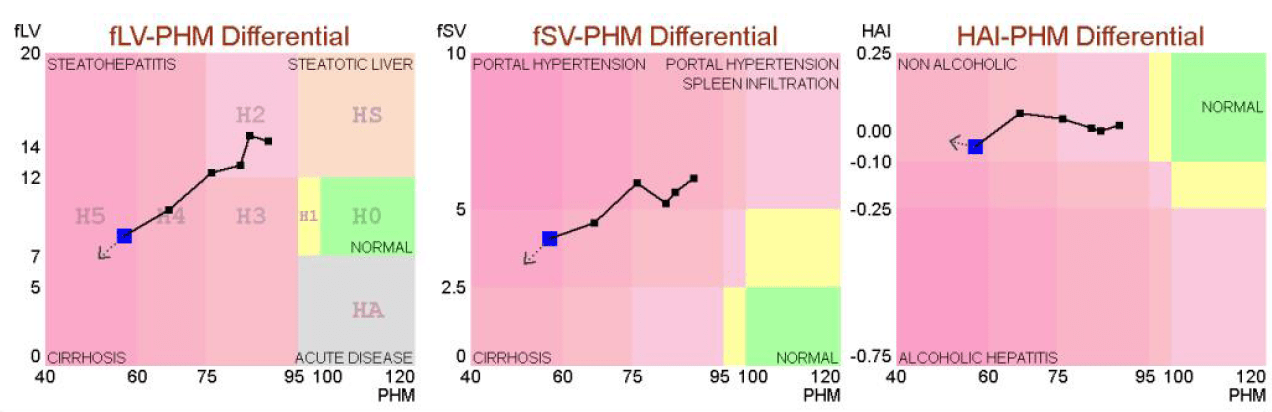
CASE 3 - H2 cirrhotic patient progressed to H5 and died. 78 year old female with decreasing PHM and fLV indicating progressive chronic liver disease. She developed ascites and died while awaiting a transplant.
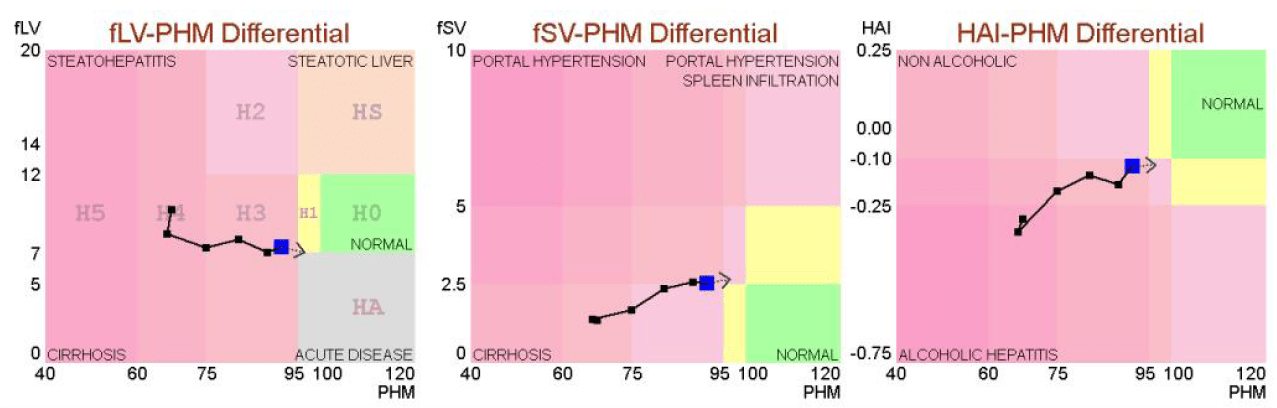
CASE 5 - H4 patient became H2 post liver transplant. 65 year old female with decompensation (H4) received a transplant liver. PHM near normal (H1) post liver transplant . Spleen volume fSV dropped indicating reduction of portal hypertension.

CASE 7 - H0 patient gaining weight at risk of MASH. 70 year old female patient gaining weight on Prednisone. Liver volume increased from 7 to 11 indicating risk of steatohepatitis. Liver function remains normal.
.png)
CASE 2 - H4 alcoholic hepatitis patient recovered to H3. 63 year old male presented with PHM 67 (H4). Patient quit alcohol and recovered to PHM 91 (H3). HAI improved from -0.30 (marked) to -0.12 (moderate).
CASE 4 - H2 patient with HCC progressed to H4 and died . 86 year old female treated three times for HCC. She developed ascites and hepatic encephalopathy after the third treatment and then died.

CASE 6 - H5 patient improved to H2 after ACAH treated. 70 year old female presented with ascites and jaundice. PHM improved from 60 to 92 after Autoimmune Chronic Active Hepatitis (ACAH) was treated with Prednisone/Immuran.

CASE 8 - F4 patient progressing from H1 to H3. 47 year old female presented as F4 cirrhosis by elastography. PHM was stable for 3 years (H1). PHM started dropping indicating risk of decompensation. Increasing fSV indicated portal hypertension.